the short read
The scan is most valuable as a systems map. It does not produce a single “do this procedure” answer. It shows anatomy that belongs in the summer intervention plan, especially the pelvic venous and varicocele track.
what is solid
Left varicocele is real on ultrasound. CT reports bilateral varicocele/hydrocele signs, mild left common iliac vein compression, and no left renal vein compression. Prostate is described as non-enlarged and homogeneous.
what is unresolved
The clinical meaning of the iliac compression is not settled. It needs symptoms, exam, duplex/venous review, and an independent vascular-andrology opinion. The current DFI status before any operation is unknown.
what not to do
Do not convert “mild compression on CT” into a stent plan. Do not convert “varicocele exists” into surgery without naming the indication: fertility, pain, testicular function, or recurrence prevention.
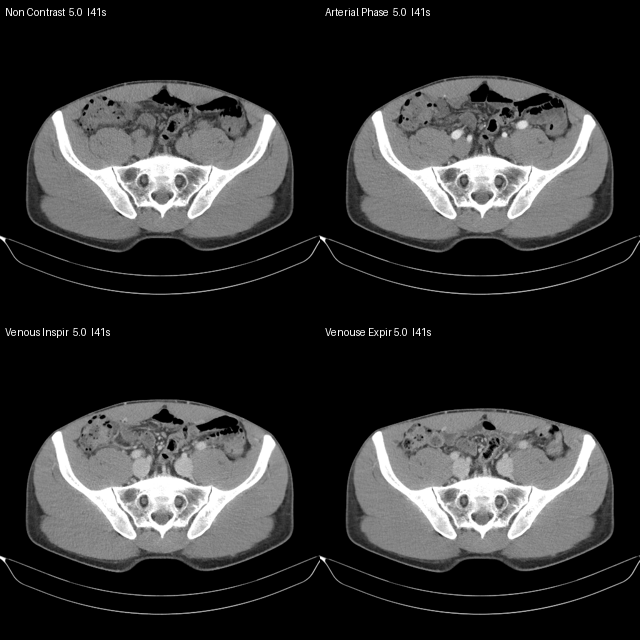
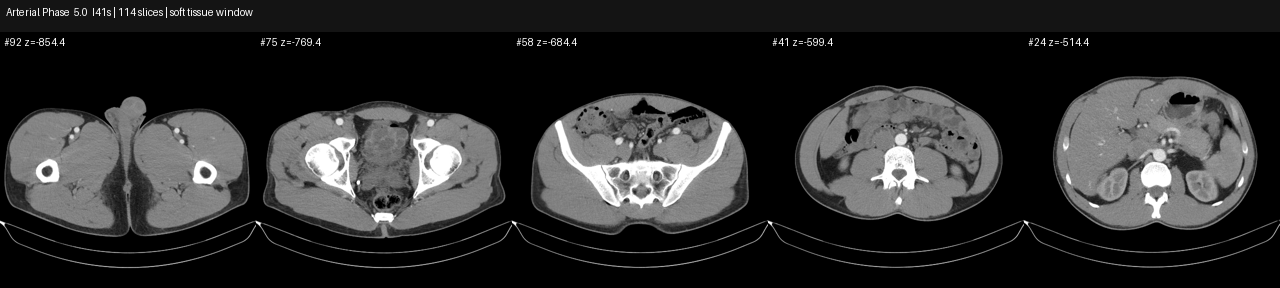
imaging orientation
The images below are de-identified preview contact sheets. They are not a radiology re-read. They show the phase structure and why this scan is useful for pelvic venous reasoning.
systems extraction
The scan touches multiple repo systems. The value is not only one vessel or one operation.
| system | what the CT contributes | decision relevance |
|---|---|---|
| pelvic venous | Mild left common iliac vein compression by the right common iliac artery at L4-L5. Iliac tunnel reported as 8 mm on inspiration and 6 mm on expiration. | Opens May-Thurner anatomy question; does not establish stent indication. |
| renal vein / nutcracker | Left renal vein is described as typical between aorta and SMA, with no compression signs. | Argues against left renal vein compression as the main varicocele driver in this report. |
| varicocele / hydrocele | CT reports bilateral varicocele/hydrocele signs; pampiniform plexus reported 5 mm right and 4 mm left. | Cross-checks ultrasound. Right side is discordant because ultrasound did not make diagnosis-forming right varicocele call. |
| fertility | The CT adds anatomy; the semen series adds function. Counts are strong, motility generally adequate, BFC morphology repeatedly low, DFI mixed across labs. | Pre-op gate should be current semen + DFI, not anatomy alone. |
| prostate / urinary | Prostate not enlarged, homogeneous structure. Paraprostatic venous plexus reported 5-6 mm. | Structural reassurance only. Does not close prostate infection/inflammation history. |
| abdominal organs | Liver, pancreas, spleen, adrenals, kidneys described without structural changes. Gallbladder removed. | Useful negative screen inside scan field; not a dedicated organ protocol. |
| lymph / bone | No enlarged abdominal/retroperitoneal/pelvic lymph nodes. No destructive/pathologic bone-density lesions at scanned level. | Gross screen reassurance, limited by report/protocol. |
may-thurner: anatomy question, not stent answer
The correct label right now is left common iliac vein compression / May-Thurner anatomy question. Syndrome and intervention require symptoms and hemodynamic significance.
- left common iliac vein compression at L4-L5
- smaller venous tunnel on expiration than inspiration
- pelvic venous plexus context exists
- wording is mild
- no DVT reported
- no collateral-severity language reported
- no pressure-gradient or IVUS significance documented
- symptom inventory is still missing
varicocele + fertility logic
The varicocele question has two layers: scrotal disease and upstream pelvic venous anatomy. They should be reviewed together, but the procedure indication must be explicit.
Ultrasound confirms left I86.1 varicocele, orthostatic, Sarteschi 3/5. This is the strongest varicocele finding.
CT reports bilateral signs, but ultrasound did not make a diagnosis-forming right varicocele call. Treat as discordant, not settled bilateral disease.
No children yet keeps fertility active. Prior conception argues against a gross absolute male-factor block. Miscarriage at 12 weeks is not automatically a varicocele signal.
| possible indication | what would make it stronger | what is missing now |
|---|---|---|
| fertility optimization | current abnormal semen/DFI trend, high DFI recurrence, unexplained infertility context, clinically significant varicocele | fresh same-method semen + DFI before surgery |
| pain | clear scrotal pain phenotype, side-specific, posture/standing relation, exam correlation | structured symptom inventory |
| testicular function | volume asymmetry/atrophy trend, endocrine or semen consequence | volume trend and andrology interpretation |
| recurrence prevention | clinically meaningful upstream pelvic obstruction | independent venous hemodynamic review |
semen series: why one snapshot is misleading
There is a real longitudinal series. The pattern is not “low sperm production.” The more relevant pattern is mixed DNA integrity, low morphology by one lab style, and recurring agglutination/aggregation.
| date | volume | concentration | total sperm | motility | morphology | DFI | read |
|---|---|---|---|---|---|---|---|
| 2025-05-15 | 7.3 ml | 189.2 M/ml | 1381.2 M | total motile 83.5% | 2.5% | 33.9% | high count; high DFI; terato/astheno + agglutination |
| 2025-07-02 | 2.2 ml | 191.2 M/ml | 420.6 M | total motile 72.5% | 3.0% | 28.0% | high count; high DFI; teratozoospermia |
| 2025-07-04 | 3.4 ml | 134.0 M/ml | 455.6 M | total motile 93.8% | 2.5% | not tested | high count; low morphology; agglutination |
| 2025-07-29 | 2.2 ml | 46.0 M/ml | 101.2 M | progressive-class b 61% | 12% | 7% | KDL normozoospermia; low DFI |
| 2026-03-06 | 3.7 ml | 163.7 M/ml | 605.7 M | total motile 60.2% | 3.0% | not tested | high count; low morphology; agglutination |
summer intervention gate
This is the action path that prevents the easiest clinic funnel from becoming the plan.
- complete symptom inventory: leg swelling, heaviness, claudication, skin changes, pelvic pain, scrotal pain, DVT history, training limits
- repeat semen analysis + DFI in a stable window
- bring CT report, DICOM manifest, scrotal ultrasound, semen series, and prior doctor call as context
- ask whether this is May-Thurner syndrome, anatomy, or neither
- ask what result would change management
- pre-commit: no diagnostic-to-stent same-session conversion
- ask whether varicocele target is fertility, pain, volume/function, or recurrence prevention
storage architecture
The repo should be the control plane, not the warehouse. Raw medical imaging is too large and too private for ordinary GitHub flow.
| layer | keep in repo | keep outside repo |
|---|---|---|
| truth | systems extraction, second opinion, decision gates, checksums, derived previews | raw DICOM, original full report bundle when not needed for packet |
| review | de-identified contact sheets, clinician packet, symptom inventory | full imaging archive for radiologist/doctor upload |
| backup | manifest and restore instructions | HealthVault / encrypted remote backup / physical source |
external anchors
These references are not a diagnosis; they anchor the decision boundaries.
- 2020 AVF/SVS/AVLS/SIR Appropriate Use Criteria: incidental/asymptomatic iliac compression stenting is rated never appropriate.
- Society for Vascular Surgery: May-Thurner syndrome: no symptoms usually means no treatment; mild symptoms may need compression; severe symptoms may need procedure.
- AUA/ASRM Male Infertility Guideline: varicocelectomy is considered for men attempting conception with palpable varicocele, infertility, and abnormal semen parameters.
This page is de-identified and omits names, exact birth date, contacts, local source paths, raw DICOM files, and original reports. It is a structured review, not medical advice.